NEWS
NEWS
NEWS
NEWS
NEWS
NEWS
NEWS
NEWS
NEWS
NEWS
NEWS
NEWS
NEWS
NEWS
NEWS
NEWS
NEWS
NEWS
NEWS
NEWS
NEWS
NEWS
NEWS
NEWS
NEWS
NEWS
NEWS
NEWS
NEWS
NEWS
NEWS
NEWS
NEWS
NEWS
NEWS
NEWS
NEWS
NEWS
NEWS
NEWS
NEWS
NEWS
NEWS
NEWS
NEWS
NEWS
NEWS
NEWS
NEWS
NEWS
NEWS
NEWS
NEWS
NEWS
NEWS
NEWS
NEWS
NEWS
NEWS
NEWS
NEWS
NEWS
NEWS
NEWS
NEWS
NEWS
NEWS
NEWS
NEWS
NEWS
NEWS
NEWS
NEWS
NEWS
NEWS
NEWS
NEWS
NEWS
NEWS
NEWS
NEWS
NEWS
NEWS
NEWS
NEWS
NEWS
NEWS
NEWS
NEWS
NEWS
NEWS
NEWS
NEWS
NEWS
NEWS
NEWS
NEWS
NEWS
NEWS
NEWS
NEWS
NEWS
NEWS
NEWS
NEWS
NEWS
NEWS
NEWS
NEWS
NEWS
NEWS
NEWS
NEWS
NEWS
NEWS
NEWS
NEWS
NEWS
NEWS
NEWS
NEWS
NEWS
NEWS
NEWS
NEWS
NEWS
NEWS
NEWS
NEWS
NEWS
NEWS
NEWS
NEWS
NEWS
NEWS
NEWS
NEWS
NEWS
NEWS
NEWS
NEWS
NEWS
NEWS
NEWS
NEWS
NEWS
NEWS
NEWS
NEWS
NEWS
NEWS
NEWS
NEWS
NEWS
NEWS
NEWS
NEWS
NEWS
NEWS
NEWS
NEWS
NEWS
NEWS
NEWS
NEWS
NEWS
NEWS
NEWS
NEWS
NEWS
NEWS
NEWS
NEWS
NEWS
NEWS
NEWS
NEWS
NEWS
NEWS
NEWS
NEWS
NEWS
NEWS
NEWS
NEWS
NEWS
NEWS
NEWS
NEWS
NEWS
NEWS
NEWS
NEWS
NEWS
NEWS
NEWS
NEWS
NEWS
NEWS
NEWS
NEWS
NEWS
NEWS
NEWS
NEWS
NEWS
NEWS
NEWS
NEWS
NEWS
NEWS
NEWS
NEWS
NEWS
NEWS
NEWS
NEWS
NEWS
NEWS
NEWS
NEWS
NEWS
NEWS
NEWS
NEWS
NEWS
NEWS
NEWS
NEWS
NEWS
NEWS
NEWS
NEWS
NEWS
NEWS
NEWS
NEWS
NEWS
NEWS
NEWS
NEWS
NEWS
NEWS
NEWS
NEWS
NEWS
NEWS
NEWS
NEWS
NEWS
NEWS
NEWS
NEWS
NEWS
NEWS
NEWS
NEWS
NEWS
NEWS
NEWS
NEWS
NEWS
NEWS
NEWS
NEWS
NEWS
NEWS
NEWS
NEWS
NEWS
NEWS
NEWS
NEWS
NEWS
NEWS
NEWS
NEWS
NEWS
NEWS
NEWS
NEWS
NEWS
NEWS
NEWS
NEWS
NEWS
NEWS
NEWS
NEWS
NEWS
NEWS
NEWS
NEWS
NEWS
NEWS
NEWS
NEWS
NEWS
NEWS
NEWS
NEWS
NEWS
NEWS
NEWS
NEWS
NEWS
NEWS
NEWS
NEWS
NEWS
NEWS
NEWS
NEWS
NEWS
NEWS
NEWS
NEWS
NEWS
NEWS
NEWS
NEWS
NEWS
NEWS
NEWS
NEWS
NEWS
NEWS
NEWS
NEWS
NEWS
NEWS
NEWS
NEWS
NEWS
NEWS
NEWS
NEWS
NEWS
NEWS
NEWS
NEWS
NEWS
NEWS
NEWS
NEWS
NEWS
NEWS
NEWS
NEWS
NEWS
NEWS
NEWS
NEWS
NEWS
NEWS
NEWS
NEWS
NEWS
NEWS
NEWS
NEWS
NEWS
NEWS
NEWS
NEWS
NEWS
NEWS
NEWS
NEWS
NEWS
NEWS
NEWS
NEWS
NEWS
NEWS
NEWS
NEWS
NEWS
NEWS
NEWS
NEWS
NEWS
NEWS
NEWS
NEWS
NEWS
NEWS
NEWS
NEWS
NEWS
NEWS
NEWS
NEWS
NEWS
NEWS
NEWS
NEWS
NEWS
NEWS
NEWS
They talk about us






Beauty chronicles

Microneedling is one of today’s most effective treatments to restore your natural glow.
8 min read

A guide to tear trough filler treatments. Discover how ART FILLER® EYES restores volume and smooths under-eye hollows for a...
12 min read

A guide to eye bag filler and dermal fillers under eyes, with insights on under eye filler before and after...
10 min read

Discover cheek fillers with hyaluronic acid dermal fillers. Learn about indications, before-and-after results for natural cheek contour enhancement.
9 min read

Learn how jawline fillers reshape the lower face, how long they last, and what to expect before and after. Read...
8 min read

Considering lip filler? Learn how it works, how long it lasts, and what to expect before and after for natural,...
9 min read

Eating a balanced diet supports gut health and nourishes your skin from within. Fillmed reveals the secrets to achieving inner...
6 min read

Discover 4 steps to help your skin regain its natural glow, along with bonus tips to purify and rejuvenate your...
7 min read

Learn how collagen and elastin impact skin ageing. Here are some solutions to boost collagen and elastin production with our...
6 min read

Hormones can affect your skin at any age, especially during key life stages like puberty, menstruation, pregnancy, and menopause. During...
6 min read

Discover expert tips to prevent and smooth neck wrinkles. Care for delicate neck skin and keep a youthful, firm neckline...
6 min read

Discover how stress impacts your skin and learn effective strategies to manage it for a youthful, radiant complexion
6 min read

You probably already heard about the “beauty sleep” concept: here is all the information you need to know about rest...
5 min read

Have you ever caught your reflection in a shop window or glanced in the mirror before heading out and noticed...
5 min read

If you’re a modern, dynamic woman on the go, you probably don’t have time for lengthy skincare routines or invasive...
6 min read
Ready to take the plunge into dermal fillers? Well done! And rest assured, when performed by aesthetic medicine professionals, the...
5 min read

You want to undergo lip injections? But before you take the plunge, you have a thousand and one questions about...
6 min read

Do you dream of having beautiful, luminous, radiant skin? You're not alone. It's a wish shared by many. In a...
6 min read

While the passage of time graces us with wisdom and experience, it also introduces us to unwelcome guests: wrinkles. Among...
7 min read
Have you noticed brown spots on your hands or face? Don't panic! These are completely normal benign skin reactions that...
7 min read

Skin ageing is a natural process that affects everyone. As we age, our skin undergoes changes: wrinkles, fine lines, age...
7 min read

Are you looking to keep your skin young and hydrated? Do you want to delay the signs of aging? Or...
8 min read

We are delighted to announce our recent achievements at the AMWC 2023 Aesthetic Medicine Awards! We received two prestigious awards:...
3 min read

Follow this guide for your dream lips: Everything you need to know before getting lip fillers.
7 min read

How can you prevent ageing skin? Ageing is a natural process that affects everyone, but that doesn't mean we have...
7 min read

There is a fine line between enough and too much when it comes to facial enhancements. We’ve all seen results...
3 min read

Discover FILLMED's Protocols FILLMED has developed a portfolio of protocols adapted to every patient and demand, from millennials to mature...
8 min read

A night to remember, Saturday 4th December. Oh, what a night, the great, the good and the beautiful were all...
3 min read

What is textured skin? A textured skin is when your face skin is uneven. It can appear without warning despite...
4 min read
What are under eye wrinkles? A wrinkle is a fold (or a ridge) in a smooth surface. It is mostly...
6 min read

THANK YOU TO ALL THE CANDIDATES. CONGRATULATIONS TO OUR 9 WINNERS. For the first time, FILLMED launched an international competition...
2 min read

IN & OUT BY FILLMED, discover our new E-magazine.
2 min read

AUTHENTIC AND SAFE BEAUTY Protect your reputation and customers. Our market is global and multi-channel, and more and more consumers...
2 min read

Be our beautiful. Be the new face of FILLMED. Become a beauty ambassador : #myNCTF casting #myNCTF casting call Be...
2 min read

There’s something about throwing out food that really bothers me. It’s not just the waste of money that stings me...
4 min read

After being in, it’s time to go out looking fresh and more hydrated. From in to out, how to face...
5 min read

We all know the benefits of getting your Zzz’s to feel and look refreshed. But did you know that what...
3 min read

You're serious about protecting yourself and others from the very real dangers of Covid-19, so you wear a mask every...
3 min read

A staycation is exactly what it sounds like. A vacation where you stay at home or around your home rather...
2 min read

Give natural, fresh, radiant results with ART FILLER® . Inspired directly from make-up artist techniques, our MEDICAL HIGHLIGHTING protocols replace...
2 min read

Skin Perfusion cabin protocols, inspired by aesthetic medicine. Your tailor-made skin rejuvenation program designed to maintain and enhance the results...
9 min read

Peeling Renew and restore your inner glow with our gluconolactone peels.
10 min read

Radiant with BioNutriGlow protocol Revitalise your natural beauty with BioNutriGlow and rejuvenate how you see yourself.
2 min read

ART FILLER® LIPS SOFT is used for the pink lip for natural enhancement...
2 min read

NANOSOFT®, the smallest needle for a new experience of injection…
2 min read

GLYCOPEEL MASK, The very latest product in the SKIN PERFUSION range...
2 min read

MEDICAL HIGHLIGHTING directly inspired from make up artist techniques to highlight the volumes and enlight the face
2 min read

Laboratoires FILLMED will be participating in all main international congresses, presenting...
2 min read

We are proud to announce the publication of the results of the 18-month clinical study on Art Filler...
2 min read
Connect & Share
 @fillmed_laboratoires
@fillmed_laboratoires
 @laboratoires-fillmed
@laboratoires-fillmed




Scientific library

1
/
35
Antioxidants, 2023 June 1
2
/
35
Journal of Cosmetic Dermatology, 2022 Jul 19
3
/
35
Journal of Dermatological Treatment, 2023 Aug 14
4
/
35
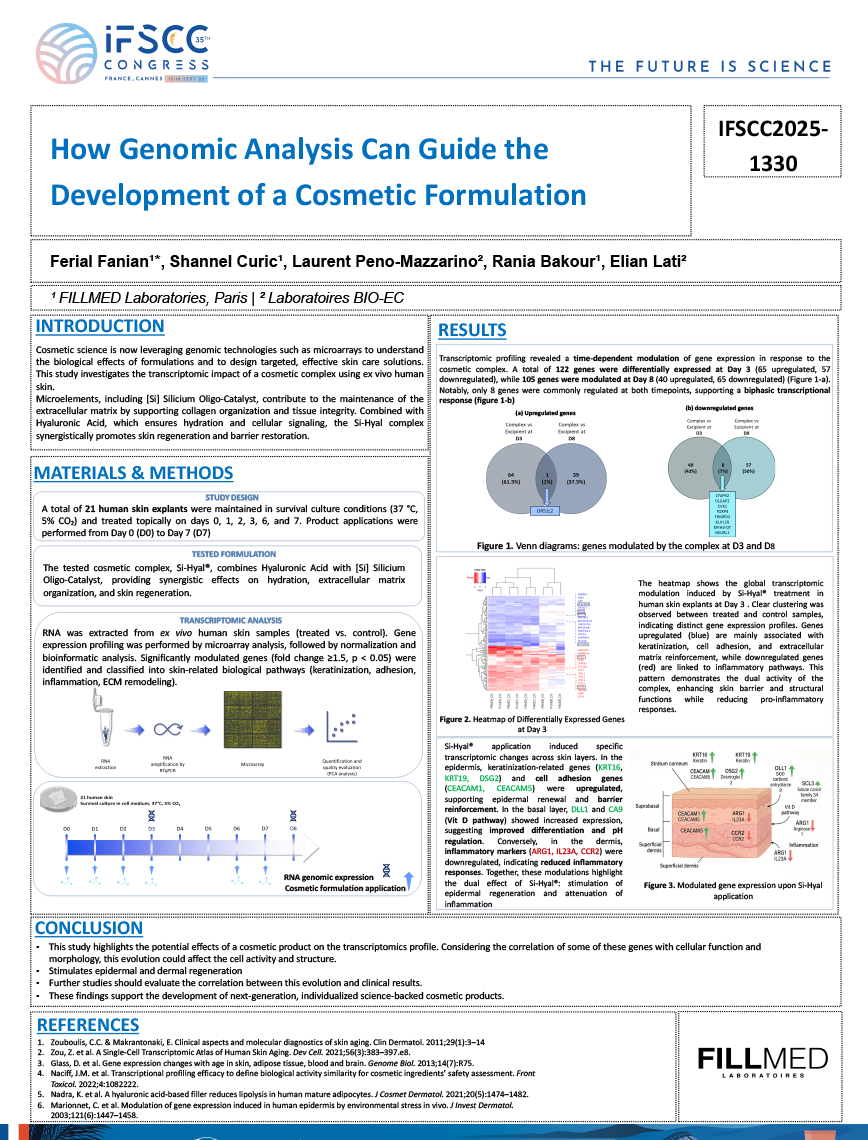
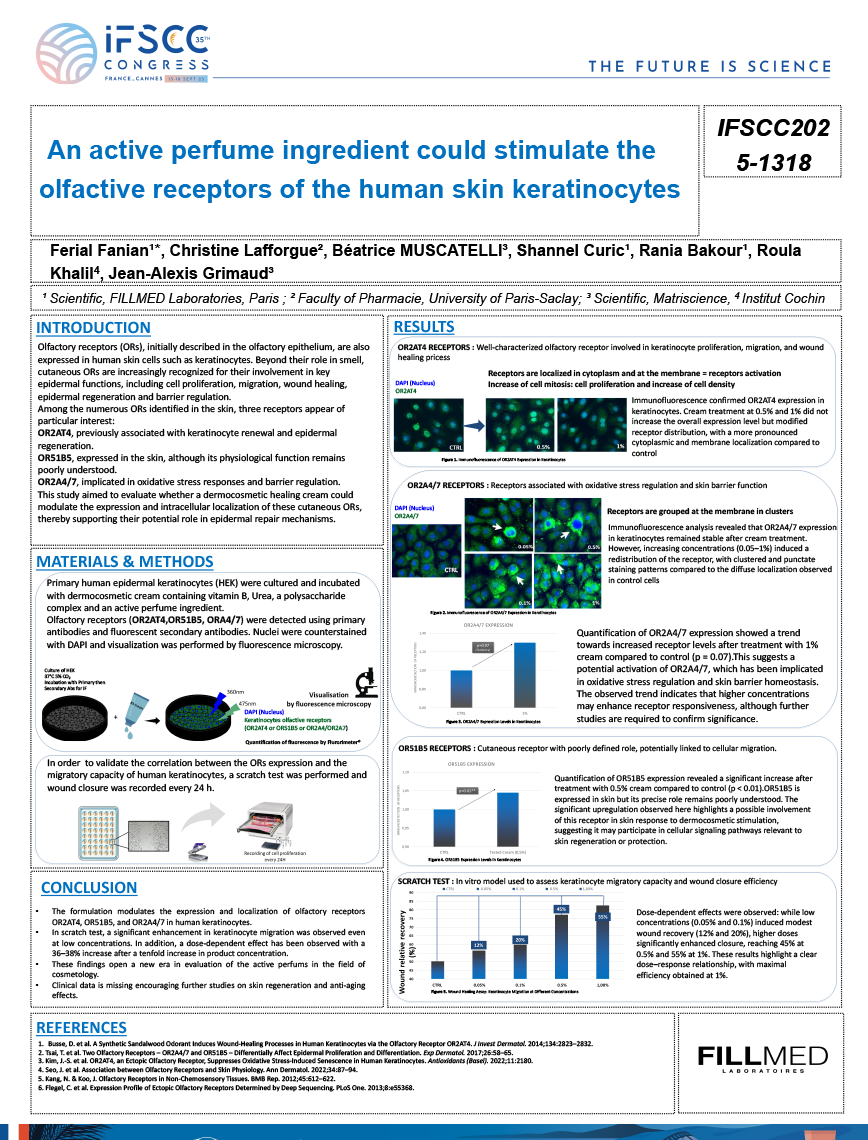
Scientific Poster exhibited during International Federation of Societies of Cosmetic Chemists Congress, Sept 2025
5
/
35
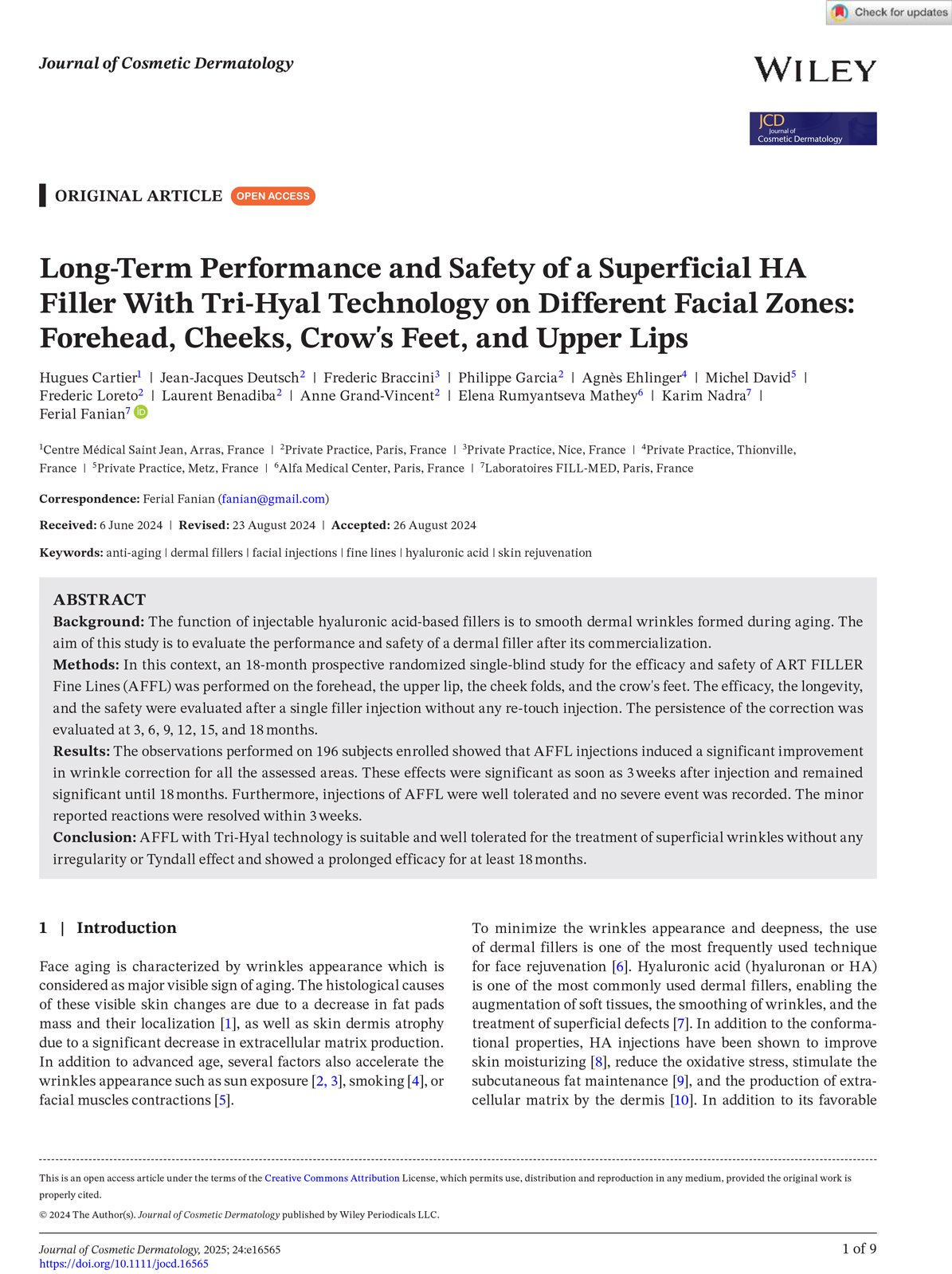
Journal of Cosmetic Dermatology, 2024, August 12
6
/
35
Journal of Cosmetic Dermatology, 2025 March 31
7
/
35
International Journal of Molecular Sciences, 2023 April 28
8
/
35
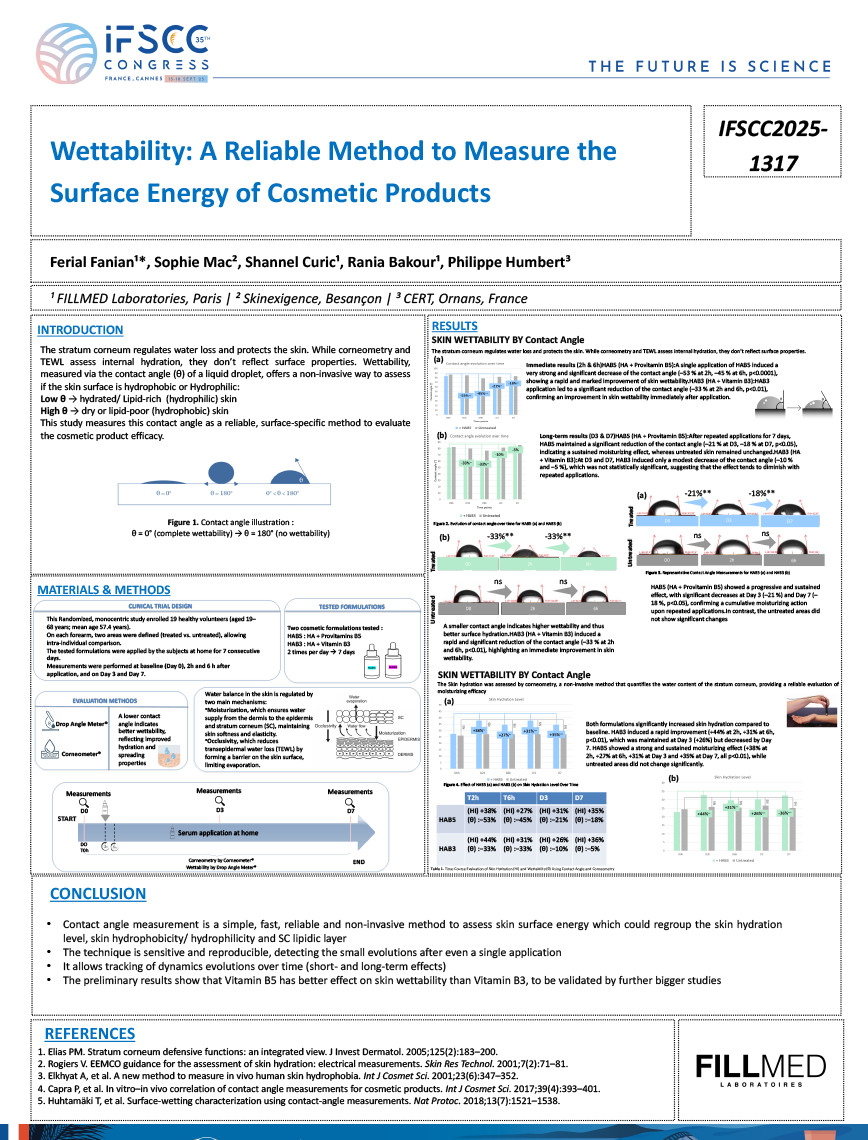
Scientific Poster exhibited during International Federation of Societies of Cosmetic Chemists Congress, Sept 2025
9
/
35
Scientific Poster exhibited during International Federation of Societies of Cosmetic Chemists Congress, Sept 2025

10
/
35
Dermatologic Surgery, 2017 Dec

11
/
35
Plastic and Reconstructive Surgery - Global Open, 2020 Dec
12
/
35
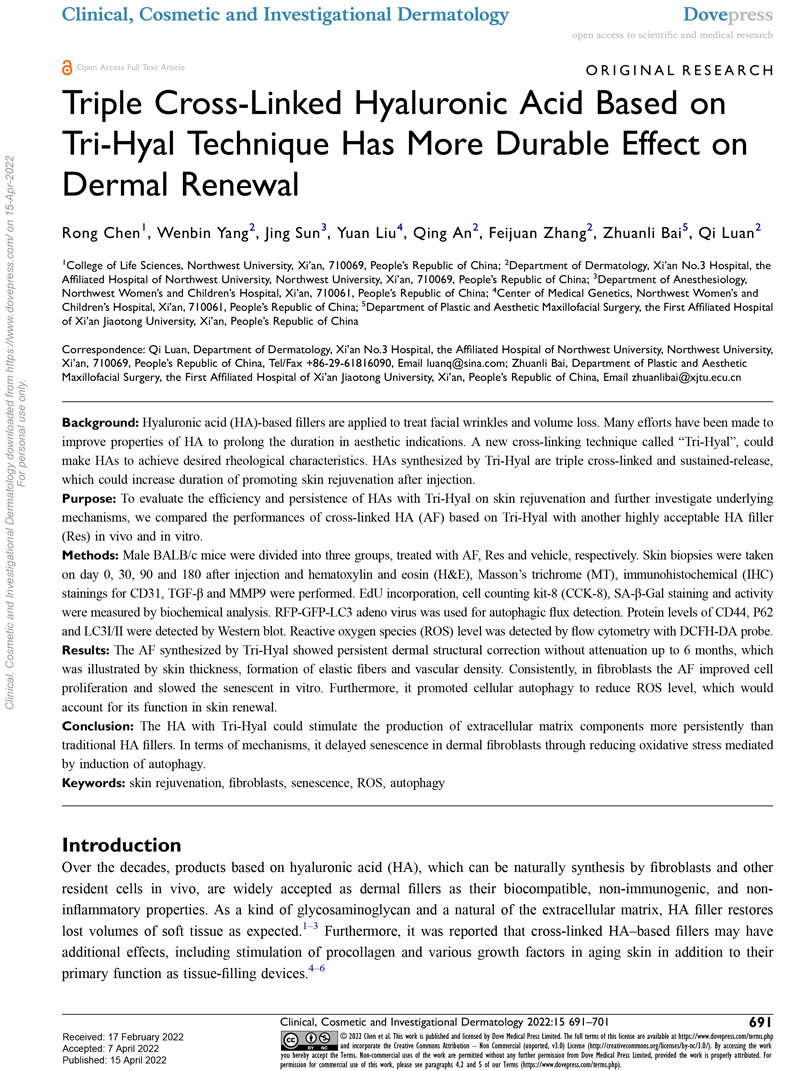
Clinical, Cosmetic and Investigational Dermatology, 2022 Apr 15
13
/
35
Journal of Cosmetic Dermatology, 2024, August 26
14
/
35
Journal of Cosmetic Dermatology, 2020 Nov 04
15
/
35
Journal of Cosmetic Dermatology, 2022 Jun 19
16
/
35
Clinical, Cosmetic and Investigational Dermatology, 2023 Jul 13

17
/
35
Journal of Aesthetic & Reconstructive Surgery, 2021 Feb 16

19
/
35
Revue de Laryngologie Otologie Rhinologie, 2017 Jan
20
/
35
Journal of Cosmetic Dermatology, 2023 May 02
21
/
35
Clinical, Cosmetic and Investigational Dermatology, 2015 Apr 7

22
/
35
Experimental Dermatology, 2011 Oct 24

23
/
35
Clinical, Cosmetic and Investigational Dermatology, 2023 Apr 24
24
/
35
Journal of Cosmetic Dermatology, 2024, September 23
25
/
35
Journal of Cosmetics, Dermatological Sciences and Applications, 2021 Mar 08
26
/
35
Official Journal of the International Union of Aesthetic Medicine UIME, 2019 Jan-Mar

27
/
35
Revue de Laryngologie - Otologie - Rhinologie, 2010 Jan 01
28
/
35
Journal of Cosmetics, Dermatological Sciences and Applications, 2017 Jan

29
/
35
The Scientific World Journal, 2020 May




35
/
35
Thieme Medical Publishers, 2023 Jul 04